


Background
Comorbid conditions, including solid and hematologic malignancies, may impact risk of contracting SARS CoV-2 or having severe COVID-19. Data specific to individual cancer types is essential to differentiate impact of patient, disease, and therapy specific factors on risk and outcomes, as the pandemic remains uncontrolled.
Goal
The primary goal of the CANDID study was to rapidly collect and analyze information on COVID-19 cases among CML pts to define prognosis, risk factors and outcome. Defining risk and predisposing features in CML patients could guide interventions, therapy modifications, and clinical management for patients and physicians.
Methods
From March 12, 2020, the iCMLf sent an anonymized case collection form to its global network of physicians treating CML pts and partner organizations. Forms were reviewed and cases tracked by an iCMLf data manager. Updates were provided weekly. Only confirmed cases or those with high level of suspicion were collected. Denominators regarding affected cohort (% tested, % affected in CML population) were not available in most instances.
Results
As of July 1, 2020, 110 cases of COVID-19 were reported to iCMLf from 20 countries: 61% from Europe, 15% from Asia, 12% from South America, 10% from North America, 2% from Africa and 1% from Oceania. COVID-19 was diagnosed by PCR and/or serology in 93 pts (85%) and clinically suspected in 17 pts (15%). Forty-six physicians reported 91 of the CML pts with COVID-19 out of a total of 12,236 CML pts that they were following (0.7%).
Median age at the time of COVID-19 diagnosis was 54 years (range: 18-89) and 55% of pts were males. Median time from CML diagnosis to COVID-19 was 7 years (range: 0-25). CML treatment at the time of COVID-19 diagnosis consisted of hydroxyurea in 1 pt (1%) and TKI in 77 (70%). Five (5%) pts were taking bosutinib, 12 (11%) dasatinib, 39 (36%) imatinib, 17 (16%), nilotinib, 2 (2%) ponatinib, 1 (1%) HQP1315 and 1 pt (1%) was treated with an unknown TKI. Eighteen (16%) pts were untreated at the time of COVID-19 diagnosis, 8 due to elective treatment discontinuation (TFR) and 10 for other reasons (toxicity (5), stem cell transplantation (1), unknown (1) and newly diagnosed CML (3)). CML treatment information was lacking at the time of cut-off in 14 cases (13%). Thirty-three (30%) cases were reported as having interrupted TKI therapy during COVID-19.
From 110 reports COVID-19 was asymptomatic in 8 cases (7%). In the 102 symptomatic pts (93%), COVID-19 was considered as mild (no hospitalization) in 49 cases (45%), moderate (hospitalization) in 19 cases (17%), severe (intensive care) in 19 cases (17%) and of unknown severity in 15 cases (14%). At the data cut-off date, COVID-19 was still active in 14 pts (13%) and outcome was unknown in 9 pts (8%). Among the 87 others, outcome was favorable in 75 pts (86%) and fatal in 12 (14%).
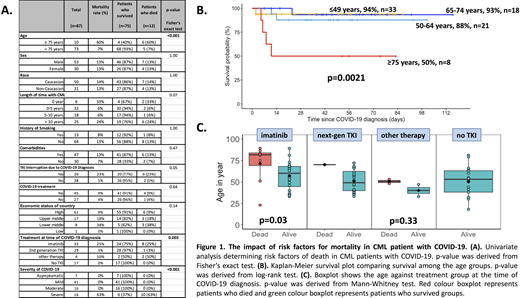
We analyzed overall survival in the 87 patients with known outcome according to sex, age, CML duration, type of CML treatment, line of TKI therapy, history of smoking, comorbidities, TKI interruption due to COVID-19, administration of any treatment against COVID-19 (antimicrobial agents, steroids, oxygen or anti-IL-6 antibodies) and economic status of country. Univariate analysis identified older age (75 vs < 75 years; mortality rate: 60% vs 7%, p<0.001), severity of COVID-19 (severe v non-severe; mortality 63% vs 0%, p<0.001) and imatinib treatment (mortality: imatinib 25% vs 2nd gen TKI 3% vs no TKI 0%, p=0.003) as predictors for COVID-19 mortality (Figure 1). Notably, 25% of imatinib treated patients were over 75years old, compared to none of the patients treated with second generation TKI.
Conclusion
The CANDID study represents the largest global cohort study to date characterizing COVID-19 in CML. Currently, the mortality rate from COVID-19 in evaluable CML patients is 13.7%. Factors associated with a higher mortality rate are age and imatinib therapy. Imatinib may represent a confounder as opposed to a true adverse prognostic predictor given the strong link between imatinib treatment and advanced age. Further case reports and longer follow up are needed to better ascertain independent risk factors, the impact of COVID-19, and the possible role that TKI type may play in this population.
Acknowledgment
The authors thank Arlene Harriss-Buchan from the iCMLf for case collection and reporting and the 61 physicians from 20 countries who contributed case reports.
Rea:Incyte: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; BMS: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees. Mauro:Bristol-Myers Squibb: Consultancy, Honoraria, Other: Travel, Accommodation, Expenses, Research Funding; Pfizer: Consultancy, Honoraria, Other: Travel, Accommodation, Expenses, Research Funding; Sun Pharma/SPARC: Research Funding; Novartis: Consultancy, Honoraria, Other: Travel, Accommodation, Expenses, Research Funding; Takeda: Consultancy, Honoraria, Other: Travel, Accommodation, Expenses, Research Funding. Cortes:BiolineRx: Consultancy, Research Funding; Arog: Research Funding; Amphivena Therapeutics: Research Funding; Astellas: Research Funding; Telios: Research Funding; BioPath Holdings: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Sun Pharma: Research Funding; Takeda: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Immunogen: Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Bristol-Myers Squibb: Research Funding; Merus: Research Funding. Pagnano:Novartis: Other: Advisory Board; Astellas: Other: Advisory Board and lecture; Pintpharma: Other: Lecture; EMS: Other: Lecture. Hughes:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Bristol-Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Foundation:Novartis: Other: Grants and sponsorship; BMS: Other: Grants and sponsorship; Pfizer: Other: Grants; Incyte: Other: Grants; Takeda: Other: Grants and sponsorship; Cepheid: Other: Grants and sponsorship.
This icon denotes a clinically relevant abstract

